Quinolone antibiotics prevent the bacteria’s DNA from unwinding, thus stopping them replicating
Quinolone antibiotics first reached the market in the 1960s, and work by preventing the bacteria’s DNA from unwinding, and thus stopping them replicating. The key target is the enzyme topoisomerase II, or DNA gyrase, and more recently introduced quinolone antibiotics such as ciprofloxacin and moxifloxacin have increased activity againt this enzyme.
However, there is a growing incidence of resistance against these key antibacterial agents; notably, the majority of strains of methicillin-resistant Streptococcus aureus are resistant to marketed quinolones. There is also significant resistance from several other bacteria, including Streptococcus pneumoniae and Pneumococcus influenzae. Therefore, there is a need for analogues of these otherwise potent antibiotics that retain activity against these resistant strains.
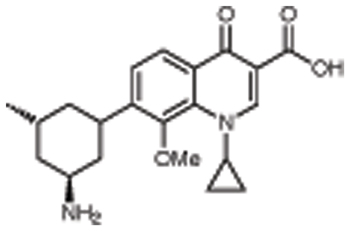
One such molecule that is under development is TaiGen Biotechnology’s nemonoxacin, which licensed the non-fluorinated quinolone drug from Procter & Gamble for development in a variety of Asian markets.1 It shows good activity against MRSA, multidrug resistant S. pneumoniae, vancomycin-resistant S. aureus and a wide range of other bacteria, both Gram positive and Gram negative.
Results of two Phase I trials have recently been published. In one 56 healthy subjects were enrolled in a double blind, ascending single dose study and randomised to one of seven dose cohorts.2 In each of these, two subjects were given placebo, and six single oral doses of between 25 and 1500mg nemonoxacin. It was well tolerated up to the maximum dose, and no serious adverse events were seen, with the most common being contact dermatitis, erythema and pruritis. Its peak time was 1 to 2 hours, and half-life between 9 and 16 hours.
In the second, 46 healthy volunteers were given oral doses of 75 to 1000mg once a day for 10 days.3 It was generally safe and well tolerated, with the most common side-effects being headache, contact dermatitis and rash. It was rapidly absorbed within 2 hours of dosing, and a steady state was achieved after 3 days in most subjects. The pharmacokinetics were affected by food, causing a decrease in plasma concentration, but free drug levels were good whether the subjects were fasting or fed.
A randomised, double blind Phase II trial has also been reported.4 Its efficacy was compared with that of levofloxacin in patients with community acquired pneumonia at once daily doses of 500 or 750mg for seven days. The most common pathogens involved were H. influenzae, S. pneumoniae and S. aureus. Clinical cure rates were 92% for the higher dose of nemonoxacin, 88% for the lower dose, and 94% for 500mg of levofloxacin. In addition, the company has recently announced by press release that it had shown promising clinical efficacy and good tolerability in a Phase II trial in patients with diabetic foot infections.
References
1. G.G. Zhanel et al. 48th Ann. Intersci. Conf. Antimicrob. Agents Chemother. Infect. Dis. Soc. Am. Ann. Meet. (Oct 25-28, Washington DC), 2008, Abst F1-2057; N. Laing et al. ibid. Abst. C1-1957
2. L. Lin et al. Antimicrob Agents Chemother. 2010, 54, 405
3. D.T. Chang et al. Antimicrob Agents Chemother. 2010, 54, 411
4. D.J. van Rensburg et al. 48th Ann. Intersci. Conf. Antimicrob. Agents Chemother. Infect. Dis. Soc. Am. Ann. Meet. (Oct 25-28, Washington DC), 2008, Abst. L-678