B-raf is a novel tyrosine kinase being investigated as a potential anticancer target. Encoded by the gene BRAF, it is involved in the Ras/Raf pathway, which passes extracellular signals to the nucleus to regulate gene expression. About 8% of solid tumours are thought to have mutated B-raf, and it is particularly common in melanoma, plus thyroid, ovarian and colorectal cancers. Many different mutations of the BRAF gene have been identified. This mutation enables the signalling pathway to pass on signals in the absence of an upstream signal, thus leading to cell proliferation.
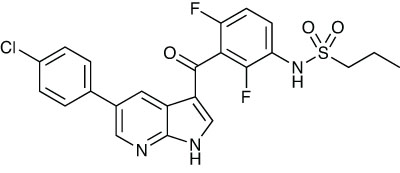
US biotech company Plexxicon is developing vemurafenib, a B-raf kinase inhibitor, in collaboration with Roche/Genentech, as a treatment for cancer, notably metastatic melanoma.1 An open label, multicentre Phase II trial was carried out in 132 previously treated patients with BRAF V600E mutation positive metastatic melanoma.2 They were given oral doses of 960mg of the drug twice a day until disease progression, unacceptable toxicity or death occurred. All had received at least one prior treatment. At the time of data analysis, 30% of patients had achieved stable disease, and 14% had had disease progression. Adverse events were generally reversible with dose modification or interrupting treatment.
In a Phase III, randomised clinical trial, it was compared with dacarbazine in 675 patients with previously untreated metastatic melanoma with the BRAF V600E mutation.3 Subjects were given either the new drug in twice daily oral doses of 960mg, or 1000mg/m2 of dacarbazine intravenously every three weeks. After six months, the overall survival in the vemurafenib group was 95%, compared with 64% for those given the control drug. An interim analysis of results by an independent data and safety monitoring board led to a crossover from dacarbazine to vemurafenib being recommended. Overall response rates were 48% for vemurafenib, compared with 5% for the control. Common side-effects with the novel agent included arthralgia, fatigue, rash, alopecia, nausea and diarrhoea, as well as squamous cell carcinoma or keratoacanthoma; 38% of patients required a dose modification because of toxic effects.
references
1. J. Tsai et al. Proc. Natl Acad. Sci. USA 2008, 105, 3041
2. A. Ribas et al. J. Clin. Oncol. 2011, 29 (suppl.), Abst 8509
3. P.B. Chapman et al. N. Engl. J. Med. 2011, 364, 2507






